
Male Infertility
About 15% of couples are infertile with 1 in 3 cases being due to male infertility. Testes produce androgens and sperm formation. Spermatogonial stem cells differentiate into mature spermatozoa in seminiferous tubules of testes.
Bone marrow and adipose derived stem cells have potential capabilities to replenish germ cells, supporting cells and testosterone producing cells hence when injected into seminiferous tubules or interstitial spaces. Bone marrow and adipose stem cells were not only able to transdifferentiate into germ cells (spermatogonia and spermatocytes) but as well as Sertoli and Leydig.
How it is done
Patients are evaluated for serum levels of gonadotrophins, testosterone and prolactine, infectious genital disease, and anatomical abnormalities of the genital tract as these issues if present need to be corrected first.
Patients advised to strictly avoid smoking, drug or alcohol consumption. As a day care procedure 240 ml of Bone marrow and 100 ml of fat is aspirated and processed for stem cells isolation. 2 ml of stem cells processed according to GMP is injected either into
- Intratesticular
- into the feeding artery of testis
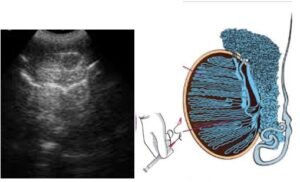
Ultrasonographic guided intratesticular injection of stem cells

Angiographic guided administration of stem cells in feeding artery of testis
What to expect
Appearance of normal healthy sperm cells at semen analysis is seen by 6 months in 60%.
- These sperms have Normal activity and possess ability to fertilise ova (validated in lab)
- Fine needle aspiration (FNA) cytology reveals evidence of differentiation and Normal intra testicular spermatogenesis
- 80 % Patients with oligospermia report significant increase (10 to 20 times) in sperm counts after 3 months of stem cell application